Recently I decided to look into the potential impact of autonomous vehicles on organ donation and found that this is a subject that many others have covered — even years ago. Surprisingly early in the history of AV development. Why this topic resulted in so many articles I don’t know. I’ve written about systemic risk and autonomous vehicles before but barely mentioned the potential impact on organ donation. However, after looking into the topic I came to the opposite conclusion of the other authors.
All the articles I found pointed to a coming shortfall of transplantable organs due to AV safety. However, I do not think that the impact will be big or even noticeable. Note that I am using a range of data I found about this, much of which seems noisy. If you have better sources or work in related industries, let me know if there are more accurate inputs that I should use.
(Note that this is different way than I usually write. In this article I’m not identifying an unintended consequence as much as I am saying that a stated one does not exist. And also note that this is a macabre subject.)
Articles on the AV and organ donor topic take a surprisingly similar view — that the coming prevalence of autonomous vehicles will result in shortages of organs for transplant. Here’s a selection of some of the more popular articles.
- “If Driverless Cars Save Lives, Where Will We Get Organs?” – Fortune
- “Self-Driving Cars Will Make Organ Shortages Even Worse” – Slate
- “What Happens If Driverless Cars Cause A Drought Of Organ Donations?” – Fast Company
- “Self-driving Cars Will Save Lives But Will They Cause Organ Shortages?” – Futurism
There are a few assumptions going into the many claims that AVs will lead to a lack of organ donation. The chief reasons are that AVs will be much safer than human drivers and will result in fewer accidents, thus resulting in fewer deaths that provide organs for transplant. However, I find these reasons to be examples of first-order (cause – effect), rather than second-order (cause – effect – and then another effect) systems thinking. And even without the systems considerations, a lack of numbers skews their conclusions.
And then again, there is a current shortage of organs for transplant, even without AVs. Is this a supply issue — not enough donors? Or is this a demand issue — too many patients because of improved techniques that enable transplants faster than supply can adjust?
![]()
It’s interesting to see that the growth in organ donors and transplants has increased well beyond population growth. But that increase is nowhere near the growth in the transplant waitlist. For these and the reasons below, I don’t believe that AVs will dramatically change the shortage of organ donations as the above articles claim.
Car accidents account for only around 15% of organ donations. The percent is a little lower if you only look at just the last 10 years, rather than the last 31 years of available data. Given that car accidents are not the major source for organ transplants, reducing this source can have only limited impact. An impact may hit certain organs more severely than others, however, as seen from this chart.
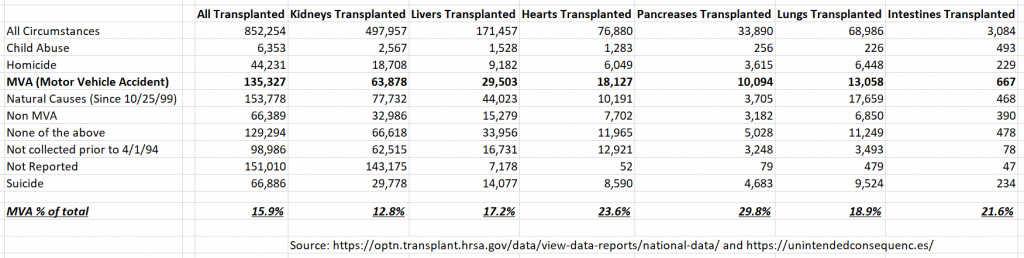
As you can see, the impact potentially hits kidneys the most — the organ that is easier for living donors since people have two. And perhaps we should discount the impact on non-essential organs (meaning you can live without them) like the pancreas, which has the highest MVA (Motor Vehicle Accident) donation rate?
Also, we should note that along with mortality rate there may be changes to which organs tend to be damaged as transportation evolves. Compare, or speculate on, the current state of driving with seat belts, airbags, and typical speed limits to the potential future AV state with different seating positions (or even prone) and faster speeds of travel.
Other measures, such as improving the opt-in rate for organ donation can have bigger impact. The US is currently at 54% opt-in while 95% of adults support organ donation. If the opt-in rate could be improved the added potential donors would be significant. If the opt-in rate were increased to the 95% referenced above (a 76% improvement), then only once AVs reduce motor vehicle fatalities by 43% (that is, reduce automotive deaths, after total opt-in, by 1/1.76) is there a break-even in potential loss of organs.

Again, this assumes the same organ recovery and transplant rate from car accidents, which may not be the case. Organ recovery post mainstream AV deployment may be higher as a percentage of accidents since the cars could report accidents immediately. Then again, if car accidents today produce a somewhat regular stream of fatalities, when AVs are mainstream the fatalities may have more peaks and valleys. That is, if AVs reduce fatalities except during times when there are major bugs or hacking events that affect large numbers of passengers. (That’s the systemic risk I wrote about in Autonomous Vehicles and Scaling Risk.) But as a way to continue to produce a supply of organs, increasing opt-in can be bigger than the safety impact, at least until a corresponding big improvement in safety.
Changes to organ donation need may exceed AV impact. Lifestyle changes, longevity, and new medical techniques may exceed the impact that AVs have. These needs may go in either direction. That is, longevity and an increase in rates of smoking may result in greater need for lungs. Or different diets plus longevity may result in the need for more hearts. Or a drop in alcohol consumption may lead to the need for fewer livers. And on and on. It’s premature to assume that the future of driving will be radically different but that health situations will not change.
Different organs are impacted differently. We have also been talking of a theoretical impact on organ donations as hitting everyone the same way. But different organs have different viability periods after host death. “Kidneys may last up to a day, while livers are limited six to 10 hours; hearts are good for perhaps four.” Again, this hits MVA organ recovery differently than living donors or donors that die from natural causes.
Changes in organ donation availability may exceed AV impact. There is a much larger source of organ availability in the greater population. While the largest source of organ transplants come from donors dying from natural causes (averaging over 40% of supply for the last 10 years), under 0.2% of natural deaths actually result in donations that go to transplants (though estimates put 1 – 2% of all deaths as meeting donation criteria). Seems like an improvement in this rate could have the largest impact overall and outstrip a shortfall caused by lower motor vehicle accidents. Since some organs may only be donated after death, improving the donation rate here also impacts certain organs (heart, lungs) more than others (kidneys, pancreas).
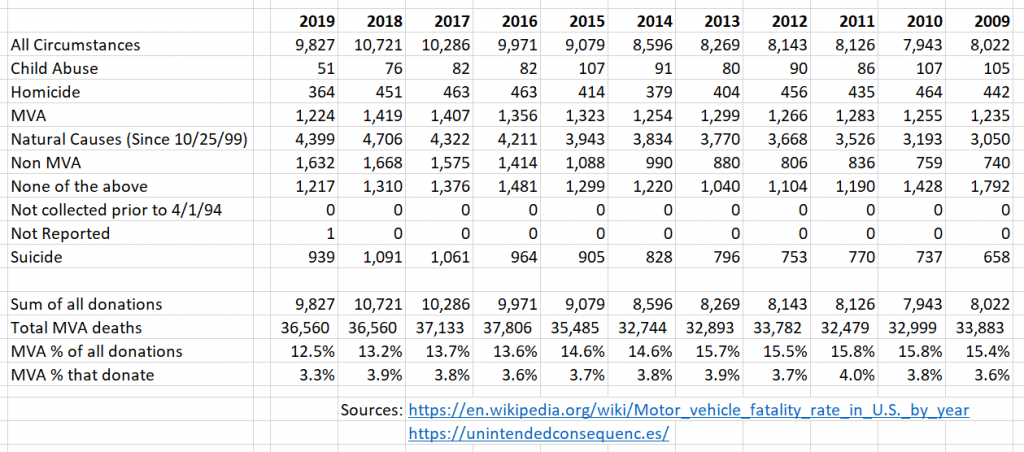
Likewise, while motor vehicle accidents account for around 15% of donated organs, those donations are only around 3.8% of those killed. Again, there is room to increase the percent of fatalities that become organ donors.
Other factors that increase the source of organs can meet the theoretical AV shortfall. The big factor here is the recent jump in drug overdose deaths in the US, like I wrote about in the Opioid Crisis article and the impact this has already had on organ donations.
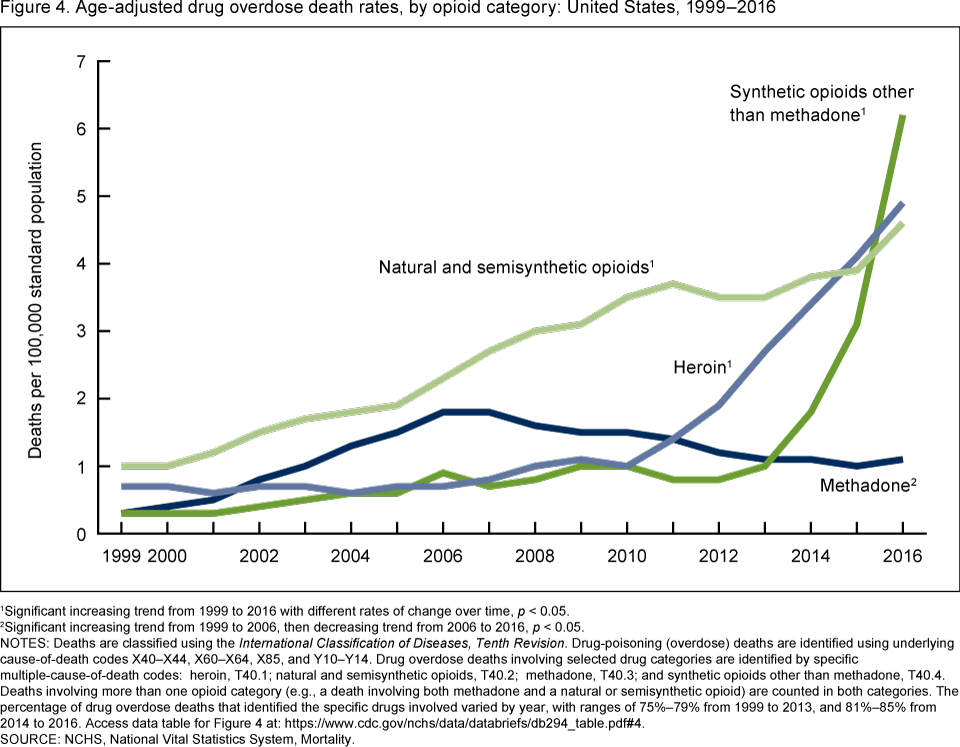
We should remember that things that can scale quickly can cause outcomes no one would expect. In the case of drug overdose deaths, the organ donors are often younger than donors that die from natural causes. And in many cases the donors are not habitual drug users, so their health isn’t terrible.
Calling a future organ shortage simply due to mainstream AVs ignores many other factors.
Consider
- If sourcing for organs changes (3D printed organs, human-animal hybrids), maybe none of this matters.
- New policies, such as payments or gifts for organs, may also make the organ shortage disappear.
- Could AV companies pioneer policies and techniques to preserve a higher percentage of motor vehicle accidents as part of their public relations? If they do indeed result in the loss of millions of jobs, could fixing the organ donor problem help their public relations? Or would that backfire?
- Without some directional numbers on how much of the organ supply comes from motor accidents and understanding flow through the system, opinions can be way off. Running some numbers gave me the differing perspective for this article. My numbers are certainly inaccurate, though I believe good enough to come to the conclusions I drew. If you have better numbers to use, contact me.